Procedures
Laparoscopy
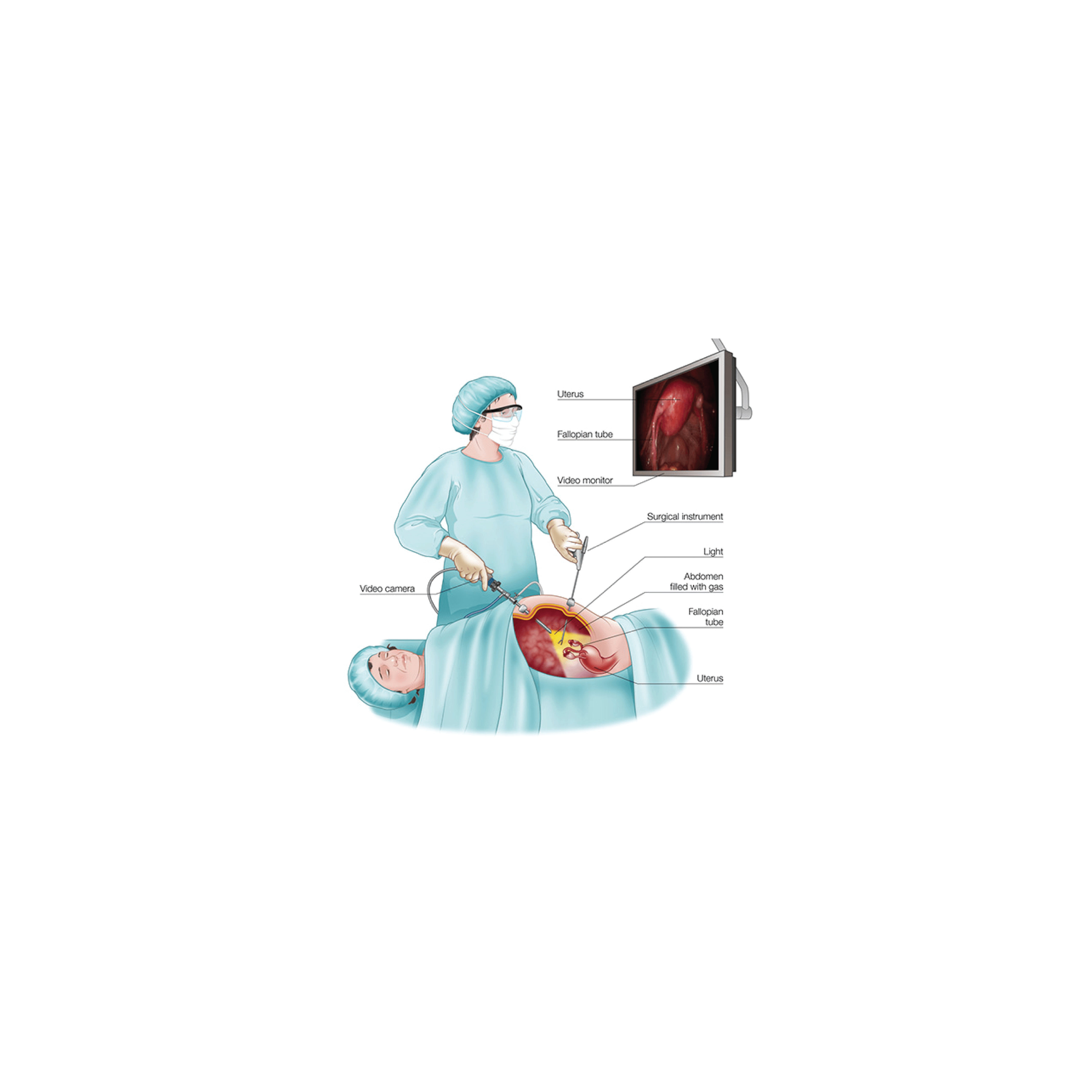
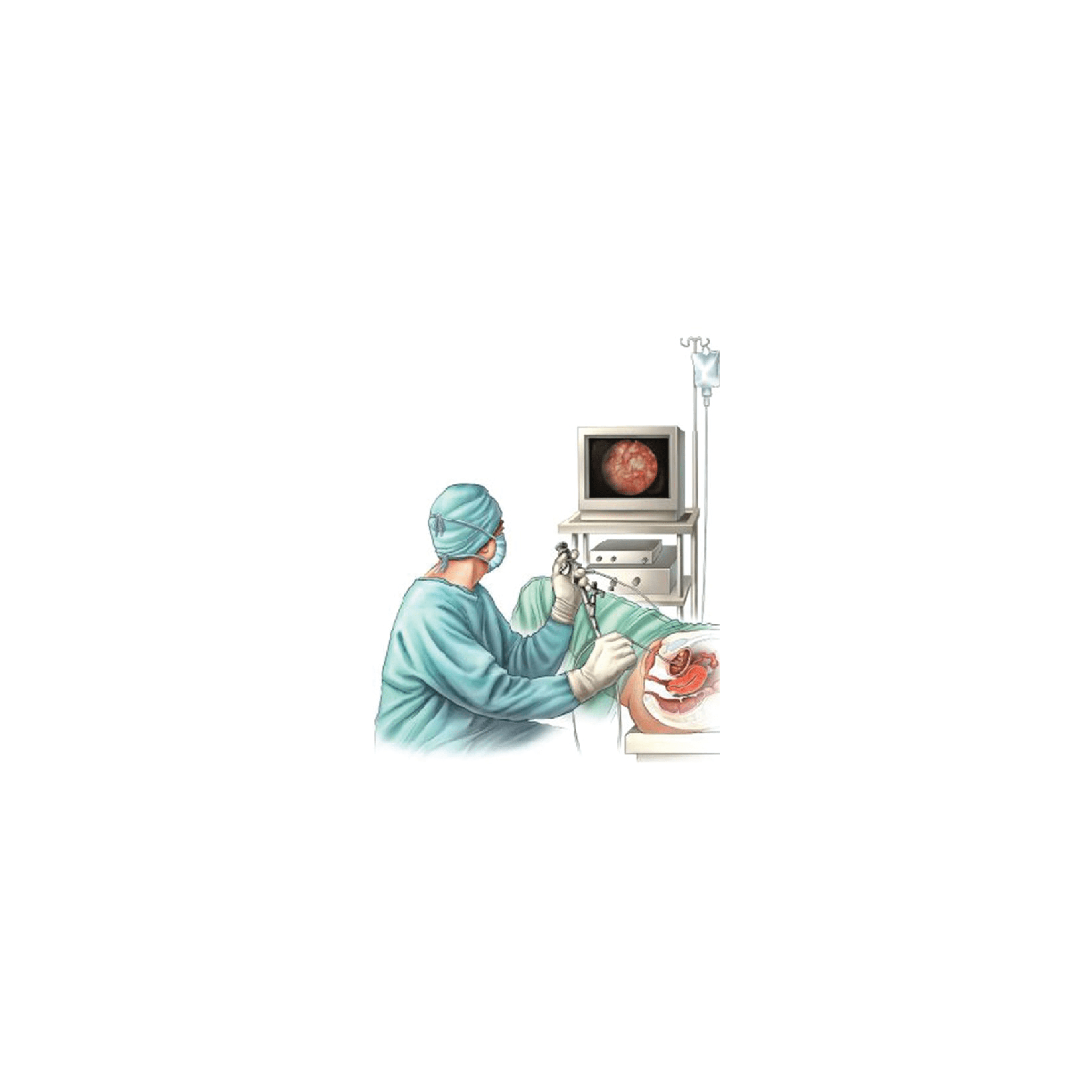
Laparoscopy is commonly called ‘keyhole surgery‘. It is a procedure in which a surgical telescope and video camera is passed through a small cut ‘keyhole‘ in the abdomen, usually in the umbilicus (belly button).
Carbon dioxide gas is used to gently inflate your abdomen during laparoscopy to enable your gynaecologist to see your pelvic organs. This allows your gynaecologist to look at, and operate on, the organs of the pelvis and abdomen. Instruments can be passed through one or more other small cuts in the wall of the abdomen.
The cuts are usually about a centimetre long so the gynaecologist can perform operations without the need for a large cut.
Laparoscopy and keyhole surgical techniques give patients a number of important advantages:
more rapid recovery
reduced pain
smaller scars
Hysterectomy
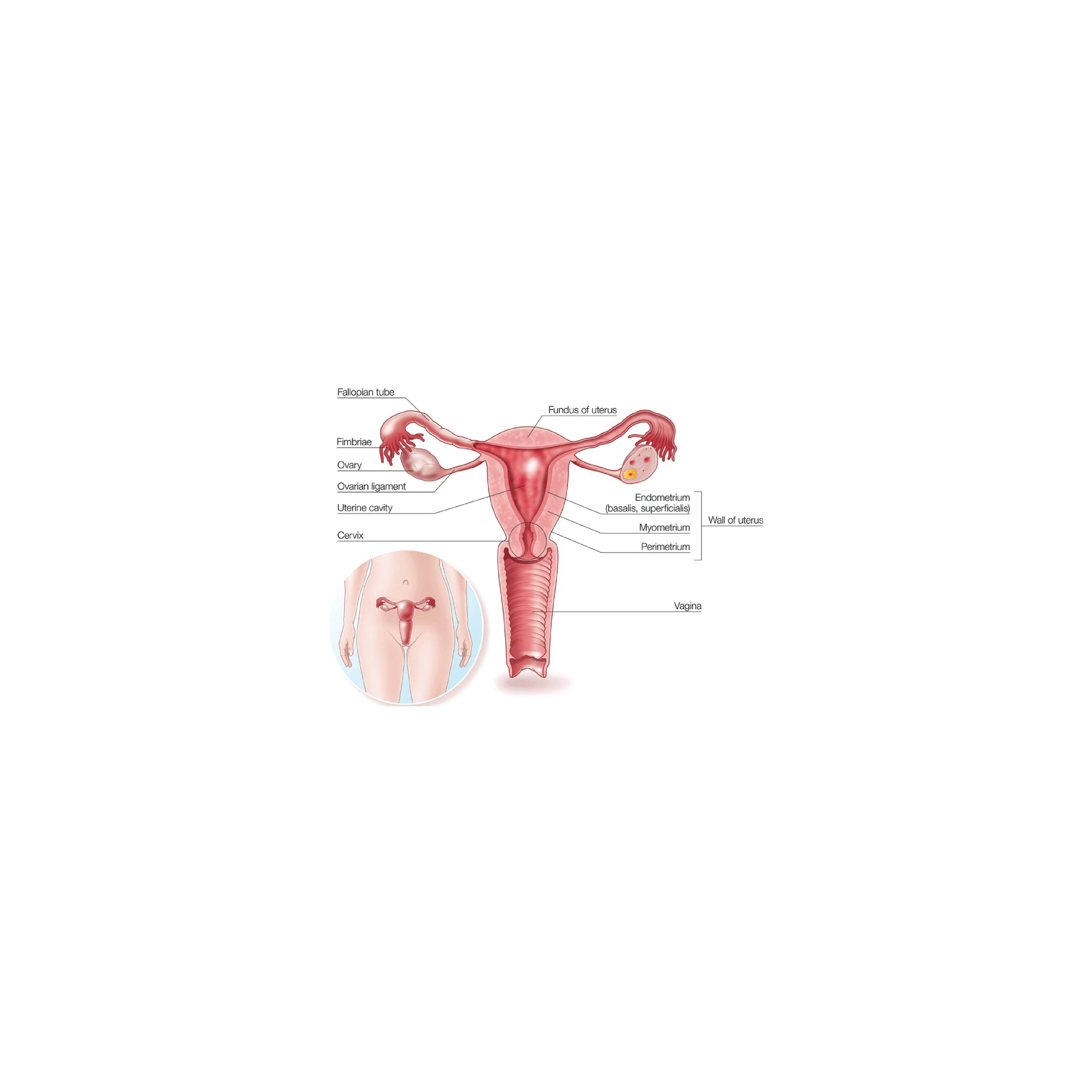
Is an operation where the uterus (womb) is removed.
There are different types of hysterectomy, and during the operation other organs, such as the ovaries or Fallopian tubes – might also be removed.
A total ‘hysterectomy’ means that the uterus and the cervix (neck of the uterus) are removed – this is the most common type of hysterectomy. A ‘subtotal‘ hysterectomy means that the uterus is removed, but the cervix is not – this is a less common operation.
At the time of hysterectomy, one or both of the ovaries might be removed. It is also common for one or both of the Fallopian tubes to be removed. It is important that you are clear about the type of hysterectomy that might be performed, and whether the ovaries or Fallopian tubes are to be removed as well.
Hysteroscopy
A hysteroscopy is a procedure used to examine the inside of the uterus (womb).
It is carried out using a narrow telescope, called the hysteroscopy, which is inserted through the cervix (opening of the womb) into the uterus. The hysteroscope is connected to a light and camera, which sends images to a monitor so that your gynaecologist is able to see inside the uterus.
As the hysteroscope is passed into your uterus through the vagina and cervix, no cut needs to be made in your skin.
Common reasons for having a hysteroscopy include abnormal bleeding, fibroids, polyps or difficulty getting pregnant.

Anterior Vaginal Repair
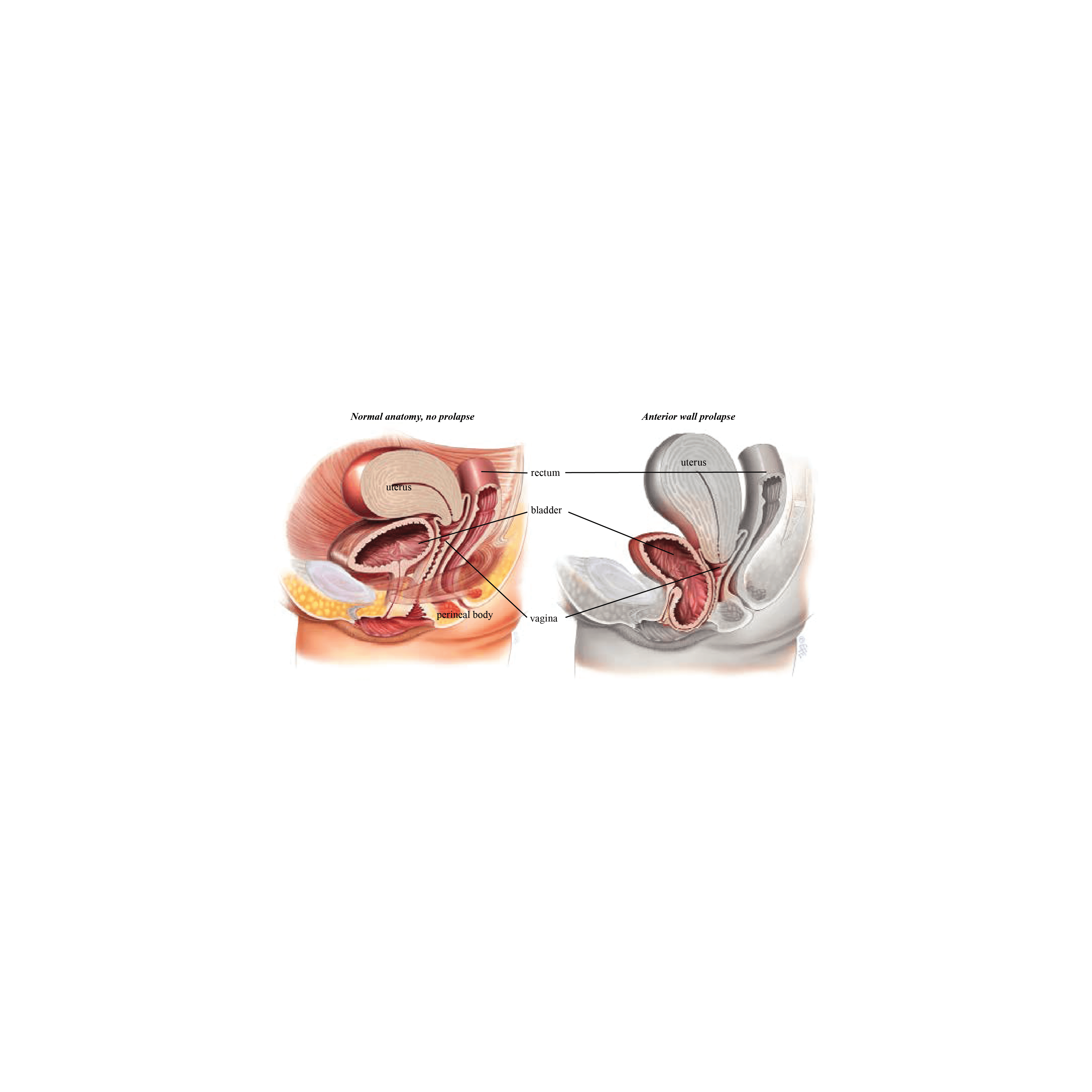
About 1 in 10 women who have had children require surgery for vaginal prolapse. A prolapse of the front (anterior) wall of the vagina is usually due to a weakness in the strong tissue layer (fascia) that divides the vagina from the bladder. This weakness may cause a feeling of fullness or dragging in the vagina or an uncomfortable bulge that extends beyond the vaginal opening. It may also cause difficulty passing urine with a slow or intermittent urine stream or symptoms of urinary urgency or frequency. Another name for an anterior wall prolapse is a cystocele.
An anterior repair, also known as an anterior colporrhaphy, is a surgical procedure to repair or reinforce the fascial support layer between the bladder and the vagina. The aim of surgery is to relieve the symptoms of vaginal bulge and/or laxity and to improve bladder function without compromising sexual function.
Posterior Vaginal Wall and Perineal Body Repair
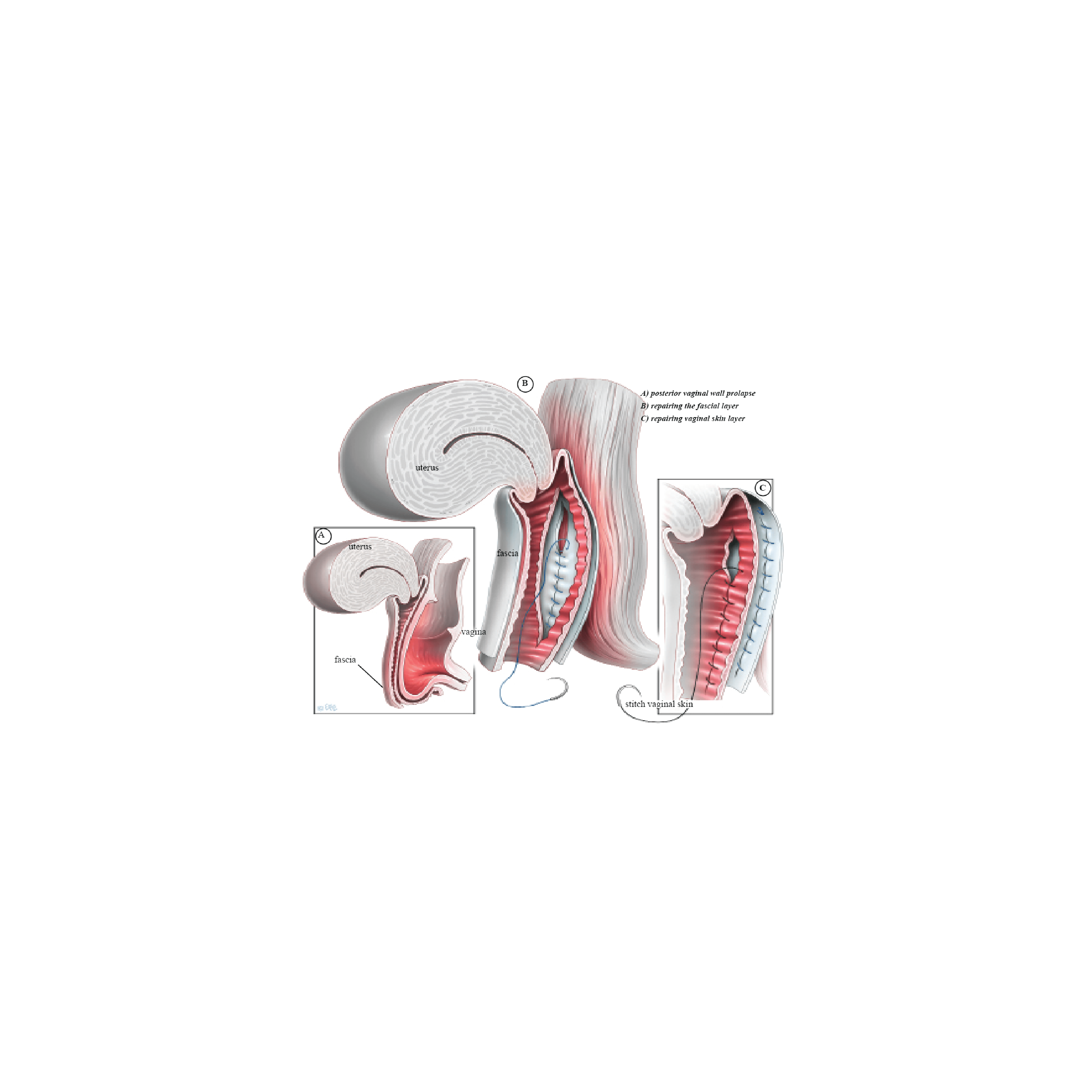
A posterior repair, also known as a posterior colporrhaphy, is a surgical procedure to repair or reinforce the fascial support layer between the rectum and the vagina. A perineorrhaphy is the term used for the operation that repairs the perineal body. The perineal body (the supporting tissue between vaginal and anal openings) also helps to support the back wall of the vagina. The perineum is the area that is often damaged when tears or episiotomies occur during childbirth. This area may need to be repaired along with the back wall of the vagina to give perineal support and in some cases reduce the vaginal opening.
About 1 in 10 women require surgery for vaginal prolapse. A prolapse of the back (posterior) wall of the vagina is usually due to a weakness in the strong tissue layer (fascia) that divides the vagina from the lower part of the bowel (rectum). This weakness may cause difficulty when passing a bowel movement, a feeling of fullness or dragging in the vagina or an uncomfortable bulge that may extend beyond the vaginal opening. Other names for the weakness of the back wall of the vagina include rectocele and enterocele.
Sacrospinous Fixation
A sacrospinous fixation is an operation designed to restore support to the uterus or vaginal vault (in a woman who has had a hysterectomy). Through a cut in the vagina, stitches are placed into a strong ligament (sacrospinous ligament) in the pelvis and then to the cervix or vaginal vault. The stitches can be either permanent or slowly absorbed over time. Eventually, they are replaced by scar tissue that then supports the vagina or uterus. This procedure is often combined with a vaginal hysterectomy and/or surgery to treat prolapse of the bladder, bowel, or stress urinary incontinence.

Cystoscopy
Cystoscopy is the name for a procedure allowing a doctor to look into your bladder and urethra with a special telescope called a cystoscope. The urethra is the tube that carries urine from the bladder to the outside of the body.
To help with diagnosis, a cystoscopy may be done to help to find the cause of symptoms such as:
Loss of bladder control (incontinence) or overactive bladder
Frequent bladder infections
Blood in the urine (hematuria)
Unusual cells found in a urine sample
Pain in the bladder, urethra or during urination
During a surgical procedure such as a hysterectomy or incontinence tape procedure to ensure there has been no damage to the bladder or the ureters
The examination is more successful than other tests, like urine tests or ultrasound, in picking up problems such as bladder stones, bleeding, tumours, and structural abnormalities of the bladder.
Two main types of cystoscopes are used: flexible or rigid. A flexible cystoscope is a thin telescope that is passed into the bladder via the urethra. It is about as thick as a pencil. Because the cystoscope is flexible, it usually passes easily along the curves of the urethra. The flexible tip can also be moved so the doctor can look at all the inside lining of the bladder and the opening of the ureters.
A rigid cystoscope is a shorter, rigid telescope. It allows a greater variety of devices to pass down side channels so that the doctor can, for example, take samples or inject into the bladder. Sometimes, it is necessary to perform a rigid cystoscopy at a later date after a flexible cystoscopy.
Caesarean Section
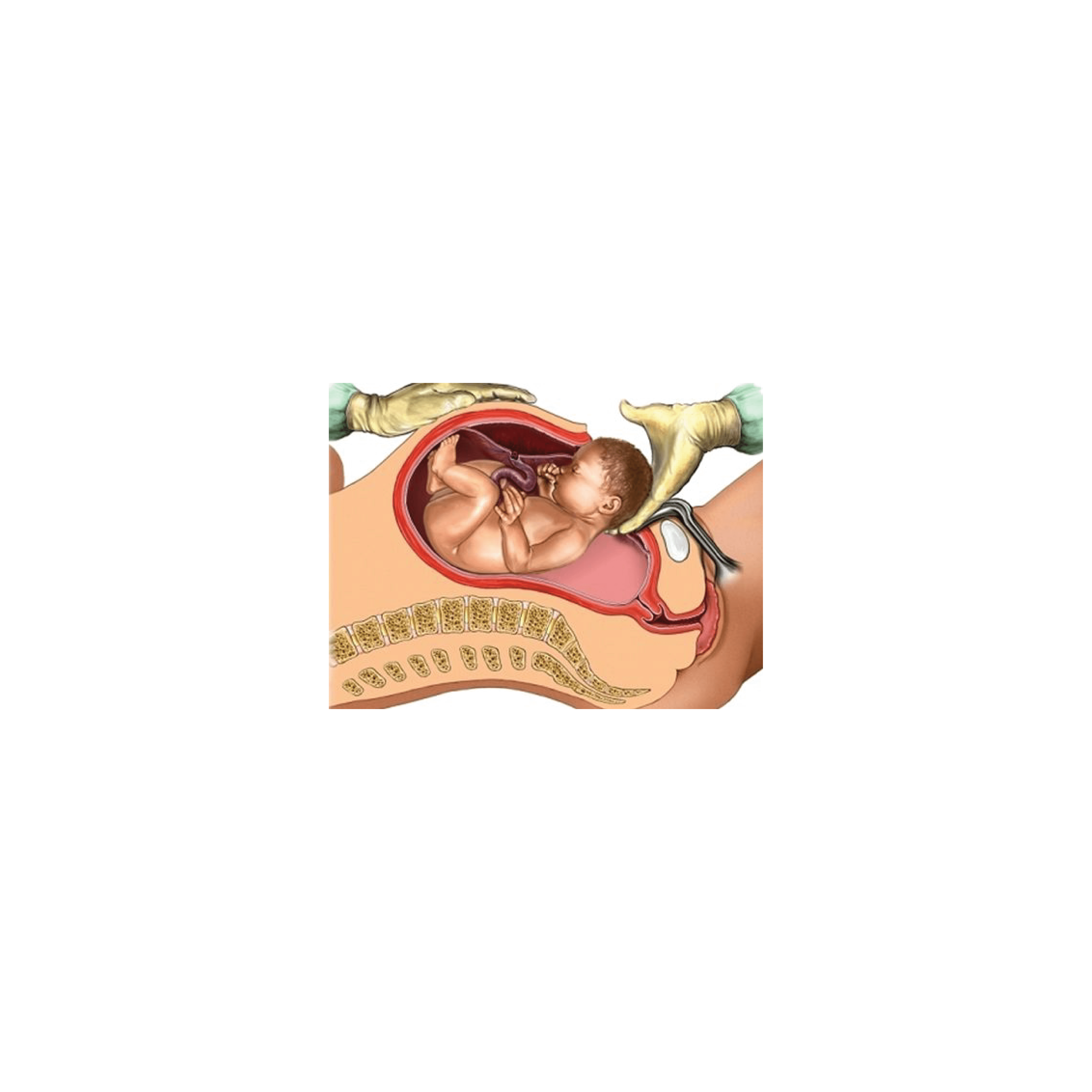
A caesarean section is an operation in which a baby is born through an incision (cut) made through the mother’s abdomen and the uterus (womb). The cut is usually made low and around the level of the bikini line.
A caesarean section may be planned (elective) if there is a reason that prevents the baby being born by a normal vaginal birth, or unplanned (emergency) if complications develop and delivery needs to be quick. This may be before or during your labour.
There are several reasons why your obstetrician may recommend an elective caesarean section. Your doctor will discuss the reason for making this decision based on your particular situation and, in some cases, your preferences.
These may include:
you have already had a number of caesarean sections.
your baby is in a breech position (bottom or feet first) and cannot be turned, or a vaginal breech birth is not recommended.
your placenta is partly or completely covering the cervix (opening to the womb).
your baby is lying sideways (transverse) and is not able to be turned by the doctor.
you have a twin pregnancy, with your first baby in a breech position.
Consult With Us
Dr Tava is dedicated to
a high standard of care
in women's health
COPYRIGHT © DR TAVA GYNAECOLOGY 2025 DESIGNED BY LITTLE BIRD CREATIVE

